Advanced In-Room Disinfection for Hospitals, Private Practice, and Surgical Outpatient Centers
Prepared by: Dr. Kris Belland, DO, MBA, MPH and Dr. Scott Trettenero, DDS
6, August 2025
AEROCLENZ.COM | 38 MILDRED DRIVE, FORT MYERS, FL 33901 | O: 239.296.9193
Introduction
Hospitals are increasingly adopting UV-C (Ultraviolet-C) light to disinfect surfaces, air, and medical equipment and help control the spread of hospital-acquired infections (HAIs) (ASHRAE, 2009). Ultraviolet germicidal irradiation (UVGI) has long been established as a means of disinfection and prevention of the spread of many infectious diseases (e.g., tuberculosis, common colds, influenza, bacterial meningitis to name a few) (Kowalski, 2009; Biasin et al., 2021).
UV-C is a specific wavelength of ultraviolet light which works by damaging the DNA or RNA of microorganisms like viruses, bacteria, and bacterial spores. It also effectively damages fungi, particularly mold and fungal spores, preventing them all from reproducing or killing them outright (de Groot et al., 2019).
The inactivating potential of UV-C light is based on damage to the RNA or DNA of viruses and bacteria and depends on the UV irradiance (UV energy per surface area). Existing studies point to UV-C’s ability to lower infection rates, cut healthcare costs, and keep workforces healthy (ASHRAE, 2009; Nerandzic et al., 2010).
Recent technological advances have enabled the production of UV-C light via light emitting diodes (LEDs). In contrast to conventional mercury vapor and xenon lamps, UV-C LEDs employ semiconductors (using AlGaN material instead of silicon) to generate targeted wavelengths. These UVC LEDs inherently produce a narrower bandwidth that resides within the UVC band, where dangers of human exposure are minimal.
UV-C LEDs are very compact with minimal heat dissipation, a long lifetime, no warm-up time, and are well suited for disinfection devices. UV-C LEDs have been shown to be equal, if not superior, to conventional UV-C mercury and xenon bulbs in effectiveness for pathogen disinfection (West, 2025). The AeroClenz AdaptUV system uses proprietary UV-C LEDs that have the highest wall plug efficiency on the market, making the system very efficient and effective.
The ceiling-mounted devices housing the UV-C LEDs are much more compact—about the size of a standard smoke detector. Easy to install, they require no special electrical configurations. Once installed, there is no staff operation or maintenance, providing a passive and continuous operational system as an additional layer for air and surface disinfection. This reduces staffing costs and time needed compared to other UV-C systems.
265nm UV-C Comparisons
The AdaptUV System includes various solutions, such as targeted air and surface disinfection and continuous upper-room disinfection, allowing for safe and effective disinfection of both occupied and unoccupied spaces. AdaptUV uses proprietary technologies and 265nm wavelength UV-C LEDs, as this has been considered one of the most effective wavelengths for disinfection since it aligns closely with the peak absorption of DNA and RNA (ASHRAE, 2009).
Why 265nm UV-C is considered “peak wavelength”:
- DNA/RNA Damage: UV-C light wavelengths range between 200–280 nm. UV-C inactivates microorganisms by damaging their DNA and RNA, preventing them from replicating and rendering them harmless. The specific wavelength of UV-C light determines how efficiently this damage occurs (ASHRAE, 2009).
- Peak Absorption at 265nm: Studies have shown that the peak absorption of UV light by a pathogen’s DNA and RNA occurs around 260–265 nm. When 265 nm UV-C light hits a pathogen’s genetic material, it is absorbed with high efficiency, leading to the formation of detrimental dimers and other disruptions that prevent replication and lead to inactivation (ASHRAE, 2009).
- Wavelength-Dependent Inactivation: Research indicates that different wavelengths within the UV-C spectrum require higher doses and longer exposure times to inactivate pathogens compared to longer wavelengths like 265 nm. This means that using UV-C LEDs tuned closely to 265 nm can achieve faster and more efficient disinfection than other wavelengths. Far-UVC (222 nm) is generally less efficient for direct DNA/RNA inactivation—research points to the need for higher dosage or longer exposure for the same kill rate in some microbes (Liu et al., 2025). 222 nm excimer lamp systems also require special bulbs that may be more expensive and have much shorter lifespans. They also generate heat and require ballasts for installation.
Healthcare Associated Infection (HAI) Mitigation
HAIs are well known to occur during hospital care—contributing to significant patient morbidity, mortality, and financial costs. It is estimated that approximately 1 in 31 hospitalized patients AEROCLENZ.COM | 38 MILDRED DRIVE, FORT MYERS, FL 33901 | O: 239.296.9193 3 has at least one HAI on any given day (Centers for Disease Control and Prevention, 2024). In 2015, the CDC estimated about 687,000 HAIs were transmitted in U.S. acute care hospitals, resulting in approximately 72,000 deaths (Centers for Disease Control and Prevention, 2024). These infections cost the U.S. healthcare system about $28.4 billion annually and can prolong hospital stays by an average of 17.6 days (about 2½ weeks) (Nerandzic et al., 2010). One in ten patients who acquire an HAI will die as a result, with HAIs now accounting for around 99,000 deaths in the U.S. (Nerandzic et al., 2010).
UV light disinfection in hospitals is proving to be crucial across various environments by providing an additional synergistic layer of protection against healthcare-associated infections. By implementing germicidal UV-C light (UVGI), hospitals can effectively inactivate pathogens on surfaces and in the air, thereby supporting stricter infection control in both clinical and common areas (Nerandzic et al., 2010; Arens et al., 2024; McDevitt et al., 2012; Walker & Ko, 2007).
By integrating the AeroClenz AdaptUV System into routine sanitation protocols, healthcare providers can reinforce disinfected environments—helping to prevent the contraction and spread of HAIs while delivering better care and confidence for both staff and patients.
In patient rooms, operating suites, procedure rooms, and surgical operatories, AdaptUV can help maintain cleanliness by neutralizing airborne and surface pathogens before, during, and after procedures.
High-traffic emergency zones are exposed to a continuous influx of patients, staff, visitors, and germs. AeroClenz AdaptUV air and surface disinfection helps reduce the microbial load in exam rooms, check-in stations, and shared seating areas, thereby curbing the spread of airborne and surface-based infections in these densely populated zones.
Restrooms are frequent sources of microbial spread due to their moist conditions and high frequency of use. AdaptUV systems can be installed near sinks, fixtures, and ventilation to help sanitize surfaces and air continuously.
UV disinfection can also be employed in hallways and elevators using upper-room UVGI fixtures. These systems sanitize circulating air while remaining safe for occupied spaces.
By implementing UV light disinfection in these key locations, hospitals strengthen their overall infection control strategy, protect vulnerable patients, and improve staff and visitor safety throughout the facility.
The AdaptUV Dual-System Approach
AeroClenz is a provider of advanced UV-C disinfection solutions for various indoor space needs. Our AdaptUV System distinguishes itself with continuous, real-time volumetric air and surface disinfection using high wall-plug efficient proprietary UV-C LED light to quickly eliminate pathogens. AdaptUV currently features a layered dual-system approach – continuous upper-room air disinfection and targeted air & surface disinfection.
Upper-room disinfection devices clean and disinfect the air above our heads, utilizing the natural flow of air convection. Airflow convection refers to the transfer of heat in a space due to temperature differences. Warm air (contaminated by people breathing, speaking, coughing, sneezing, etc.) rises to the UV-C halo and will be disinfected continuously. HVAC produces cooler, filtered air which will be cleaned by the upperroom device. This disinfected air will sink, providing a constant source of fresh, clean air.
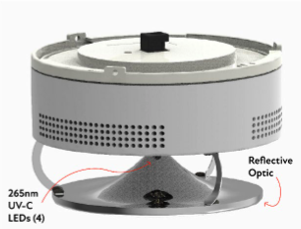
Upper-room disinfection devices emit UV-C light in the upper portion of high-traffic areas, such as patient rooms, corridors, and waiting areas, safely out of the reach of occupants. Studies, including a clinical TB trial, demonstrate that upper-room UVGI can reduce tuberculosis transmission by approximately 70–80% in high-risk indoor hospital settings (Mphahlele et al., 2015). CDC and NIOSH widely recognize UVGI in their official UVGI guidelines as a proven airborne infection control strategy (Centers for Disease Control and Prevention & National Institute for Occupational Safety and Health, 2009).
Our upper-room disinfection devices can become part of a layered approach with existing induct UV-C systems. Hospitals often incorporate UV-C into air handling systems to continuously inactivate airborne pathogens and prevent microbial buildup on HVAC components. UV lamps used in HVAC systems, furnaces, and air conditioning systems help to enhance indoor air quality (IAQ), providing cleaner, healthier air in hospitals and healthcare facilities (Air Movement and Control Association International, 2020). When used together, upper-room and in-duct UVGI can offer a layered approach to infection control, removing airborne contaminants in occupied spaces and treating recirculated air.
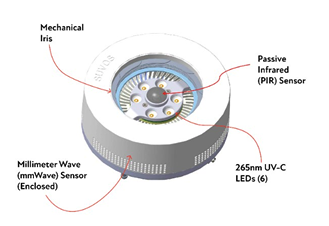
Our targeted air & surface disinfection devices utilize six powerful yet safe UV-C LEDs to provide a targeted cone of disinfection—neutralizing pathogens wherever the light reaches. These proprietary devices are equipped with multiple internal human-presence sensors, making them safe, effective, and efficient. The newest advancements have synergistic effects with chemical disinfectants and other conventional disinfection procedures, improving hygiene and environmental sustainability while reducing risk via redundant fail-safe engineered systems.
Millimeter Wave (mmWave)
This patented and proprietary technology is an integral aspect of the AdaptUV system. It incorporates mmWave radar sensors operating at 24 GHz, providing highly accurate and reliable detection of human presence within its disinfection range. mmWave sensors emit highfrequency electromagnetic waves and measure the time it takes for these signals to reflect after hitting an object, providing precise detection and ranging of objects. This sensing technology continuously monitors spaces—out of an overabundance of caution, AeroClenz ensures the UV-C LEDs are automatically deactivated and the mechanical iris is safely closed whenever human presence is detected. With a wide detection field of view, the mmWave efficiently recognizes both stationary and moving individuals, significantly enhancing the safety and effectiveness of disinfection processes in hospital environments.
Passive Infrared (PIR) Sensor
In addition to mmWave sensing, the device also features a PIR sensor. PIR sensors detect infrared radiation naturally emitted by humans by sensing changes in heat signatures within their detection zone. This dual-sensor approach ensures redundancy and increases reliability in human-presence detection. The PIR sensor effectively complements the mmWave system by detecting thermal radiation emitted by humans, disabling UV-C operation when individuals approach within its 2-meter direct detection range.
Together, the mmWave and PIR sensors create a highly responsive, safe, and intelligent device capable of dynamically adapting its operation based on human activity. No other UV-C system on the market has this sensing capability. The device operates in distinct modes. It enters disinfection mode when no human presence is detected, opening the mechanical iris and activating the UV-C LEDs for a predefined disinfection cycle lasting a full uninterrupted 10 minutes. 10-minute cycles are programmed into the device to ensure higher log reductions against more resilient pathogens, such as fungal spores.
Upon completion of the cycle, it transitions to standby mode, with the iris safely closed, until human presence is detected again. This intelligent mode-switching ensures optimal disinfection efficiency while prioritizing safety, energy efficiency, and staff-free operation.
The AeroClenz Difference
UV-C disinfection in hospitals is becoming increasingly important but is also increasingly differentiated among available options—mercury vapor bulbs, excimer lamps (KrCl* excimer UV, 222 nm), and UV-C LEDs. UV-C LEDs emit around 260–280 nm wavelengths, which have proven effective at inactivating pathogens while avoiding harmful byproducts, unlike older technologies that emit a wide range of UV wavelengths. Utilizing the 265 nm wavelength with redundant sensors provides maximal safety by constraining intensity and eliminating other harmful and unnecessary wavelengths.
UV-C technology delivers superior disinfection efficacy at a potentially lower investment compared to HEPA filters, ionization systems, and other UV-C solutions such as UV robots. Incorporating UV-C robots into existing hospital workflows may require significant adjustments to staffing schedules and protocols. User interfaces may not always be intuitive, necessitating staff training and potentially frequent technical interventions. Robots may need reprogramming if furniture or other objects are moved, impacting autonomous functions. The AdaptUV system needs no staff intervention or maintenance, reducing staffing costs and time.
UV-C LED technology is mercury-free and considered more environmentally friendly than traditional UV lamps. Mercury lamps are being discontinued or eliminated in accordance with the Minamata Convention on Mercury. UV-C LEDs have a superior lifespan of up to 15,000 hours, resulting in lower replacement costs annually than non-LED systems (United Nations Environment Programme, 2013).
AeroClenz offers custom-designed systems using proprietary UV-C technology to continuously inactivate airborne and surface pathogens, providing effective and safe disinfection for any facility. Other systems, like robots, require staff to spend time and energy scheduling and setting up equipment. Also, with robots and many other UV-C systems, disinfection is only accomplished either before or after procedures.
We have differentiated ourselves through our emphasis on continuous, real-time, and safe UVC LED disinfection, particularly in sensitive environments like hospitals. Our focus on advanced sensor technology to ensure safety in occupied spaces—combined with our commitment to delivering effective disinfection solutions—are key differentiators within the UVC LED market.
Conclusion
Hospitals today face mounting challenges in ensuring patient safety, reducing hospitalacquired infections (HAIs), and maintaining operational efficiency in increasingly complex environments. UV-C LED disinfection technology offers a powerful, science-backed, and environmentally conscious tool to meet these demands head-on. By effectively eliminating pathogens in both air and on surfaces, UV-C LED systems help prevent infections before they start, reducing the length of hospital stays, improving patient outcomes, and restoring confidence in healthcare environments.
The AeroClenz AdaptUV System represents a significant leap forward in this effort. Unlike legacy solutions that require manual deployment or involve operational disruptions, AdaptUV is fully automated, maintenance-free, and safe for continuous use in occupied spaces. Equipped with dual-redundant occupancy sensors (mmWave radar and PIR), the system ensures human safety while delivering real-time disinfection. Its 265 nm UV-C LEDs operate at the peak germicidal wavelength, maximizing efficacy while minimizing energy use, maintenance demands, and environmental impact.
Hospitals implementing this technology are not only improving infection control but also reducing associated costs, streamlining workflows, and strengthening environmental stewardship by eliminating the need for mercury-based systems and the overuse of chemical disinfectants. From patient rooms and surgical suites to emergency departments and public restrooms, the AdaptUV system can be seamlessly integrated to bolster existing infection control strategies.
Recent findings support UV C LED disinfection as a viable and effective addition to existing infection prevention strategies. Integrating the AdaptUV System into clinical workflows provides continuous air and surface inactivation, complementing traditional cleaning methods without disrupting patient care. This approach aligns with current evidence emphasizing multi layered disinfection strategies as a means to reduce pathogen exposure for patients and staff.
This patented and proprietary UV-C LED technology is presently being brought to the market through AeroClenz. For more information on this exciting new technology, visit www.AeroClenz.com/medical.
Bibliography and Further Reading
- Air Movement and Control Association International. (2020, October). UV-C for HVAC air and surface disinfection. https://www.amca.org/educate/articles-andtechnical-papers/amca-inmotion-articles/uv-c-for-hvac-air-and-surface-disinfection2.html
- West, G. F. (2025, May). A validation experiment: Utilizing ultraviolet light to disinfect high-use nursing equipment. American Journal of Infection Control, 53(5), 548–551. https://doi.org/10.1016/j.ajic.2024.12.017
- ASHRAE. (2009). Ultraviolet air and surface treatment (Chapter 62). In 2019 ASHRAE Handbook—Applications. https://www.ashrae.org/file%20library/technical%20resources/covid-19/ip_a19_ch62_uvairandsurfacetreatment.pdf
- Biasin, M., et al. (2021, October). Robust evaluation of ultraviolet-C sensitivity for SARS-CoV-2 and surrogate coronaviruses. International Journal of Molecular Sciences, 22(16), 9131. https://pubmed.ncbi.nlm.nih.gov/34668746/
- Centers for Disease Control and Prevention. (2024, November). Healthcareassociated infections: Reports and data. Retrieved from https://www.cdc.gov/healthcare-associated-infections/php/data/index.html
- Centers for Disease Control and Prevention, & National Institute for Occupational Safety and Health. (2009, March). Ultraviolet germicidal irradiation guidelines for healthcare settings. https://www.cdc.gov/niosh/docs/2009-105/default.html
- de Groot, T., et al. (2019, March). Killing of Candida auris by UV‐C: Importance of exposure time and distance. Mycoses, 62(7), 665–670. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6850319/
- Liu, Q., et al. (2025). Disinfection efficacy and safety of 222-nm ultraviolet C compared with 254-nm ultraviolet C: Systematic review and meta-analysis. Journal of Hospital Infection, 161(1), 55–67. https://doi.org/10.1016/j.jhin.2025.04.004
- McDevitt, J. J., Rudnick, S. N., & Radonovich, L. J. (2012). Aerosol susceptibility of influenza virus to UV-C light. Applied and Environmental Microbiology, 78(6), 16661669. https://doi.org/10.1128/AEM.06960-11
- Mphahlele, M., et al. (2015, August). Institutional tuberculosis transmission: Controlled trial of upper-room ultraviolet air disinfection—a basis for new dosing guidelines. American Journal of Respiratory and Critical Care Medicine, 192(4), 477–484. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4595666/
- Nerandzic, M. M., et al. (2010, June). Applications of ultraviolet germicidal irradiation disinfection in health care facilities: Effective adjunct, but not stand-alone technology. American Journal of Infection Control, 38(5, Suppl 1), S13–S24. https://www.ajicjournal.org/article/S0196-6553(10)00420-7/fulltext
- United Nations Environment Programme. (2013). Minamata Convention on Mercury. Retrieved from https://www.mercuryconvention.org
- Kowalski, W. (2009). Ultraviolet germicidal irradiation handbook: UVGI for air and surface disinfection. Springer.
- Walker, C. M., & Ko, G. (2007). Effect of ultraviolet germicidal irradiation on viral aerosols. Environmental Science & Technology, 41(15), 5460–5465. https://doi.org/10.1021/es070056u
Download the AdaptUV System Medical Whitepaper as a PDF:


